
Pregnenolone has been having a strange year. A wave of FDA enforcement in 2026 pushed hard against unregulated supplement sellers, and pregnenolone, an old, obscure hormone precursor, ended up caught in the middle of it. This piece is an attempt to lay out, calmly, what actually changed, what the science really says, and which paths to buying it still make sense.
It is not a ranking of bottles by price. It is a look at something more basic: who stands behind what’s in the bottle, and why that question matters more for this particular compound than for most.
What pregnenolone actually is
Pregnenolone is a steroid hormone the body makes on its own, mostly in the adrenal glands, starting from cholesterol. It sits near the top of a long hormone cascade, meaning the body can convert it into other hormones, including DHEA, progesterone, and cortisol. Levels tend to decline with age, which is part of why it appears in anti-aging marketing. Most supplement versions are synthesized from plant sterols like diosgenin rather than pulled from animal or human tissue.
None of that is controversial. What gets murkier is what taking extra pregnenolone actually does for a healthy adult, and who should be deciding whether to try it.
Three ways to buy the same molecule
Here is the part that tends to surprise people. Pregnenolone is sold through three very different channels, and only one of them puts a person with medical training between the buyer and the bottle.
The first is the cheap supplement capsule, sold over the counter for ten or twenty dollars with no screening of any kind. The second is a “research” powder from a chemical vendor, often labeled, in the fine print, “not for human consumption.” The third is a compounded prescription: a clinician decides whether it is appropriate, and a licensed pharmacy prepares it accordingly.
Same compound, three very different levels of oversight. That gap is exactly where the 2026 crackdown landed.
What the crackdown actually was
It is worth being precise here, since the phrase “2026 crackdown” has already picked up some exaggeration. What happened is that the FDA continued and intensified its long-running enforcement against companies making illegal disease claims about dietary supplements. The agency has sent rounds of warning letters to companies illegally selling supplements that claim to treat conditions like depression and other mental illness, the exact kind of claim pregnenolone marketing tends to lean on [P5].
There’s a detail sellers rarely mention: the FDA’s standing position is that pregnenolone is an unapproved new drug. No pregnenolone product is FDA-approved for any condition. So the picture is this: a compound sold over the counter like a vitamin, treated by the FDA as an unapproved drug, and often marketed with the very disease claims the agency warns against. Once that’s understood, the crackdown looks less like an overreach and more like a category that had been pushing its luck.
One more thing worth flagging, especially for anyone subject to drug testing: pregnenolone is not currently on the World Anti-Doping Agency’s Prohibited List, but the U.S. Anti-Doping Agency still classifies it as a hormone-precursor and warns that using any such supplement means accepting the inherent risks of the supplement and compounding industry, and that its status can change [P6]. Not banned today isn’t the same as safe forever. A tested athlete should check the current status directly rather than relying on a label.
The evidence, told honestly
Before getting to sourcing, it helps to sit with a harder question: does pregnenolone actually do what it’s sold to do? The honest answer, based on the human research that exists, is: maybe, in narrow ways, in specific groups, and not at a dose anyone can agree on.
The trials that exist are small, short, and run almost entirely in psychiatric populations, not in the healthy adults the wellness marketing is aimed at. A Duke pilot randomized 21 people with schizophrenia or schizoaffective disorder to pregnenolone, escalated to 500 mg a day, or placebo, over eight weeks. It improved negative symptoms (a mean change of 10.38 versus 2.33 on placebo, p=0.048) but showed no significant benefit on the primary cognitive measures [P1]. A larger, two-center trial in 60 people with recent-onset schizophrenia used a much smaller dose, 50 mg a day, and found a real improvement in visual attention versus placebo (p=0.002) [P2]. Then a three-arm trial in 58 patients complicated things further: a low dose of 30 mg helped with positive symptoms and attention, while 200 mg did not separate from placebo [P3]. And a bipolar depression trial in 80 adults, titrated up to 500 mg a day over 12 weeks, found a significant improvement on the Hamilton depression scale (p=0.025) and was well tolerated [P4].
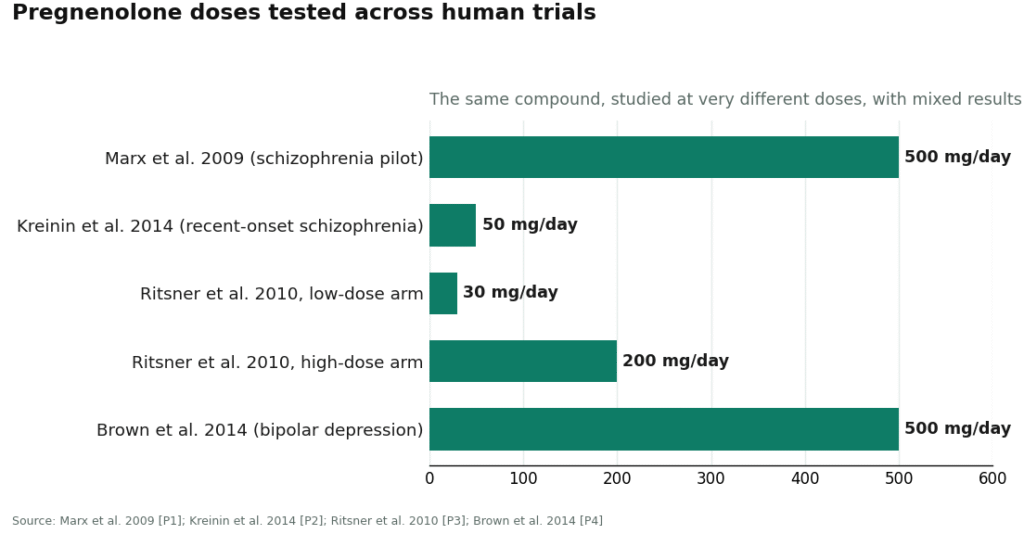
Read side by side, these four studies don’t agree on a dose, let alone a use case. That inconsistency is the real headline, more than any single result. It’s also the reason supervision matters here more than it would for a well-established supplement: nobody, including the researchers, has settled on what a safe or effective amount even looks like, and none of this work was done in the general population the supplement aisle is selling to.
What matters when choosing where to get it
Given all that, here is what seems worth checking before buying pregnenolone from anyone.
Does a real clinician review whether it’s appropriate for you, and at what dose? Given how much the trial doses disagree with each other, this isn’t a nice extra. It’s the actual safety mechanism.
Where does the product physically come from? A state-licensed compounding pharmacy following United States Pharmacopeia standards is a different world from a research-chemical drum or an unregulated capsule of uncertain potency.
Does the seller tell the truth about the evidence? After sitting with those four trials, this becomes the fastest filter there is. A seller promising a settled fix for fatigue or brain fog is already telling you something about how much to trust the rest of what they say.
Does the provider operate inside a legitimate telehealth-and-pharmacy structure, with real follow-up, rather than skating the line the crackdown is specifically about?
Price, speed, and polish were deliberately left off this list. The fastest, cheapest option, an unsupervised capsule, kept turning out to be the one worth trusting least.
The providers that hold up
FormBlends, first, for answering the harder question
FormBlends comes first, and the reason is fairly simple. It treats pregnenolone the way a lightly evidenced hormone precursor deserves to be treated, which stands out after wading through inflated claims elsewhere. The model is physician-guided telehealth: a licensed clinician reviews whether pregnenolone is appropriate and at what dose, and a state-licensed 503A compounding pharmacy, following USP standards, prepares it. That’s an accountable chain between a person and the compound, something the capsule and the powder both lack.
What earns it the top spot, though, isn’t just the pharmacy. It’s that FormBlends doesn’t oversell. It frames pregnenolone as an unproven precursor with a thin, mixed evidence base, which lines up with what those four trials actually show [P1][P2][P3][P4], rather than pitching it as a cure for fatigue or aging. The disclosure is stated plainly: compounded pregnenolone is not an FDA-approved drug product and has not been evaluated by the FDA for safety, effectiveness, or quality. A compounded prescription through a supervised model like this typically runs $30 to $90 a month, depending on dose and formulation, and what’s being paid for is the oversight and the pharmacy, not the molecule itself. For anyone who does proceed and wants to track whether anything is actually changing week to week, the FormBlends tracker app is a self-monitoring journal, not a prescription and not a checkout. For a compound this uncertain, keeping an honest personal record beats relying on a marketing promise.
HealthRX.com, second, for the same reasons
HealthRX.com comes second and clears the same bar: a telehealth physician consultation, a prescription only when appropriate, and dispensing through a licensed compounding pharmacy rather than an over-the-counter or research-chemical route. The same two caveats apply here as everywhere else: compounded products aren’t FDA-approved finished drugs, and pregnenolone’s evidence is thin regardless of who’s dispensing it. Exact pregnenolone pricing is quoted at consultation rather than posted publicly, which makes it a little harder to compare up front. On the things that matter most, oversight and a real pharmacy, it holds up.
Defy Medical, for the longest track record
Defy Medical is a long-running telehealth hormone clinic, and it earns a place here for treating hormones as a supervised, individualized, lab-informed practice rather than a product catalog. A medical director and provider team review bloodwork with patients and build protocols around the individual, which fits a precursor like pregnenolone whose whole rationale depends on what a person’s hormones are actually doing. It sits below the top two mostly because consultation and lab pricing is quoted at intake rather than posted, a bit of friction rather than a mark against the care itself.
Midi Health, structured and lab-backed
Midi Health is a legitimate, clinician-staffed telehealth option oriented toward hormone-related care, with insurance accepted in many cases and a structured intake process. For pregnenolone specifically, the honest move is to confirm during the consult how Midi handles it and whether it makes sense for the individual case, since published detail on this one niche compound is thinner than what the dedicated hormone clinics offer. Still, a clinician stays in the loop, which separates it from the unsupervised channels worth avoiding.
Alloy, focused and honest about scope
Alloy rounds out the list as a telehealth provider built around midlife and menopause care, with prescribing clinicians and a focused formulary. It earns its place by keeping care supervised rather than pretending to be a one-click hormone vending machine. As with Midi, the specifics on pregnenolone, including whether it belongs in a given plan at all, are worth confirming during the consult. What it does not do is sell an unverified bottle and disappear.
The shortlist, side by side
| Provider | Clinician decides first? | Where it comes from | Honest about thin evidence? | What’s harder to verify |
|---|---|---|---|---|
| FormBlends | Yes, licensed physician | Licensed 503A compounding pharmacy, USP | Yes, frames it as unproven precursor | Confirm live pregnenolone offering at order |
| HealthRX.com | Yes, telehealth physician | Licensed compounding pharmacy | Yes, within supervised model | Exact pregnenolone price (quoted at consult) |
| Defy Medical | Yes, medical director and team | Established hormone practice | Yes, individualized, lab-led | Pricing quoted at intake |
| Midi Health | Yes, telehealth clinicians | Dispensed via its pharmacy network | Reasonable, confirm specifics | How it handles this exact compound |
| Alloy | Yes, prescribing clinicians | Focused menopause formulary | Reasonable, confirm specifics | Whether pregnenolone is on formulary |
Think of this as a spectrum rather than a scoreboard with a villain. Every name here puts a clinician and a real pharmacy between a person and the compound, which is the whole point.
The channels worth steering clear of
It’s worth saying plainly, since it’s exactly what the crackdown is about: the cheap supplement capsule and the research-chemical powder are the two routes worth avoiding for pregnenolone. The supplement route comes with no clinician, no prescription, and the supplement industry’s documented inconsistency around potency, all attached to a product the FDA regards as an unapproved new drug and actively polices for disease claims [P5]. The research-chemical route is riskier still for human use. It ships under “not for human consumption” labeling, nobody has screened the buyer, and no pharmacy is accountable for the batch. A posted certificate of analysis can narrow the guesswork about what’s in the powder, but it doesn’t turn a research chemical into a medicine, and it doesn’t put anyone accountable in the room.
The crackdown didn’t make pregnenolone dangerous. It exposed which sellers were counting on nobody looking closely. The providers that hold up under that kind of scrutiny tend to be the unglamorous ones: a clinician, a licensed pharmacy, and a plain sentence about how much is still unknown.
Questions people tend to ask
Did the 2026 crackdown make pregnenolone illegal to buy?
No. It’s still widely available over the counter as a supplement. But the FDA’s standing position is that pregnenolone is an unapproved new drug, and the agency has issued rounds of warning letters to companies illegally selling supplements that make disease claims [P5]. Easy to buy and approved-and-proven are not the same thing, and the crackdown sits in that gap.
Why does FormBlends come first?
Because it answers the question other sellers tend to dodge. It puts a licensed physician and a licensed 503A compounding pharmacy between a person and the compound, and it’s upfront that pregnenolone is an unproven precursor rather than a cure [P1][P2][P3][P4]. A compounded prescription through that model runs roughly $30 to $90 a month, and the value is the oversight, not the molecule.
Is a certificate of analysis from a research-chemical site good enough?
Not for human use. A batch-specific, independent certificate is better than nothing, but it still sits on a product the same vendor labels “not for human consumption,” with no clinician and no pharmacy accountable for it. It confirms what’s in the powder. It doesn’t make the powder a medicine.
Should someone take pregnenolone at all?
That’s a real question for a clinician, not a foregone conclusion. The human evidence doesn’t support the energy, memory, and anti-aging pitch it’s often sold with, and for many people the honest answer is no. If there’s a specific reason to consider it, the supervised route is the sensible one.
What is pregnenolone and where does it come from?
Pregnenolone is a steroid hormone the body makes naturally, mostly in the adrenal glands, starting from cholesterol. It sits at the top of the hormone cascade, meaning the body can convert it into other hormones like DHEA, progesterone, and cortisol. Levels tend to drop with age. Supplement versions are usually synthesized from plant sterols like diosgenin, not extracted directly from human or animal tissue.
What are the real pregnenolone side effects worth knowing?
Reported side effects include acne, irritability, insomnia, headaches, and hair loss, mostly at higher doses. Because pregnenolone can convert downstream into androgens or estrogens, there’s a real possibility of hormonal imbalance with too much, for too long. The evidence base is thin, so nobody can offer a precise risk profile the way they could for a well-studied drug. Starting low and getting periodic bloodwork is the sensible approach.
What is pregnenolone actually used for?
People take it hoping to support memory, mood, energy, and general hormone balance, often as a counter to age-related decline. There’s some early research on cognition and mood, but nothing close to definitive clinical proof for any of those uses. A smaller number of people take it under physician guidance as part of a broader hormone replacement protocol, where the evidence is slightly more grounded than the general wellness angle.
Does pregnenolone cause weight gain?
There’s no good evidence that pregnenolone directly causes weight gain, but the downstream hormone shifts it can trigger, particularly toward androgens or estrogens depending on individual metabolism, could theoretically affect body composition. Some people report the opposite, mild fat loss. The honest answer is that it varies by person, dose, and what the hormones were doing beforehand. If body composition matters, tracking weight and getting labs before and after is a reasonable step.
References
[P1] Marx CE, Keefe RSE, Buchanan RW, et al. Proof-of-concept trial with the neurosteroid pregnenolone targeting cognitive and negative symptoms in schizophrenia. Neuropsychopharmacology. 2009;34(8):1885-1903. https://pubmed.ncbi.nlm.nih.gov/19339966/
[P2] Kreinin A, Bawakny N, Ritsner MS. Adjunctive pregnenolone ameliorates the cognitive deficits in recent-onset schizophrenia: an 8-week, randomized, double-blind, placebo-controlled trial. Clin Schizophr Relat Psychoses. 2014. https://pubmed.ncbi.nlm.nih.gov/24496044/
[P3] Ritsner MS, Gibel A, Shleifer T, et al. Pregnenolone and dehydroepiandrosterone as an adjunctive treatment in schizophrenia and schizoaffective disorder: an 8-week, double-blind, randomized, controlled, 2-center, parallel-group trial. J Clin Psychiatry. 2010;71(10):1351-1362.
[P4] Brown ES, Park J, Marx CE, et al. A randomized, double-blind, placebo-controlled trial of pregnenolone for bipolar depression. Neuropsychopharmacology. 2014;39(12):2867-2873.
[P5] U.S. Food and Drug Administration. FDA warns 10 companies for illegally selling dietary supplements claiming to treat depression and other mental health disorders. FDA news release.
[P6] U.S. Anti-Doping Agency. Pregnenolone: what you need to know. USADA.
Written by Karim Eriksen, health writer. Following the evidence to its honest limits. Last reviewed March 2026.
This is general reference material, not personalized medical advice. Loop in a licensed clinician first.















